The diagnosis of tinea corporis is usually clinical and should pose no problem to the physician provided the lesion is typical, but can be difficult with prior use of medications, such as calcineurin inhibitors or corticosteroids. Background Tinea corporis is a common fungal infection that mimics many other annular lesions. Physicians must familiarize themselves with this condition and its treatment. Objective This article aimed to provide a narrative updated review on the evaluation, diagnosis, and treatment of tinea corporis. Methods A PubMed search was performed with Clinical Queries using the key term ‘tinea corporis.’ The search strategy included clinical trials, meta-analyses, randomized controlled trials, observational studies, and reviews. The search was restricted to the English language. The information retrieved from the mentioned search was used in the compilation of the present article. Results Tinea corporis typically presents as a well-demarcated, sharply circumscribed, oval or circular, mildly erythematous, scaly patch or plaque with a raised leading edge. Mild pruritus is common. The diagnosis is often clinical but can be difficult with prior use of medications, such as calcineurin inhibitors or corticosteroids. Dermoscopy is a useful and non-invasive diagnostic tool. If necessary, the diagnosis can be confirmed by microscopic examination of potassium hydroxide wet-mount preparations of skin scrapings from the active border of the lesion. Fungal culture is the gold standard to diagnose dermatophytosis especially if the diagnosis is in doubt and results of other tests are inconclusive or the infection is widespread, severe, or resistant to treatment. The standard treatment of tinea corporis is with topical antifungals. Systemic antifungal treatment is indicated if the lesion is multiple, extensive, deep, recurrent, chronic, or unresponsive to topical antifungal treatment, or if the patient is immunodeficient. Conclusion The diagnosis of tinea corporis is usually clinical and should pose no problem to the physician provided the lesion is typical. However, many clinical variants of tinea corporis exist, rendering the diagnosis difficult especially with prior use of medications, such as calcineurin inhibitors or corticosteroids. As such, physicians must be familiar with this condition so that an accurate diagnosis can be made and appropriate treatment initiated.
Emergence of Trichophyton mentagrophytes as the Predominant Pathogen in Tinea Corporis: A Clinico-Etiological Study from Southern India, PDF, Fungus
Management of tinea corporis, tinea cruris, and tinea pedis: A comprehensive review
PDF) Tinea Corporis, Caused by Microsporum Canis - a Case Report From Kosovo
Notes from the Field: First Reported U.S. Cases of Tinea Caused by Trichophyton indotineae — New York City, December 2021–March 2023
PDF) Tinea corporis: An updated review
PDF) Tinea corporis: An updated review
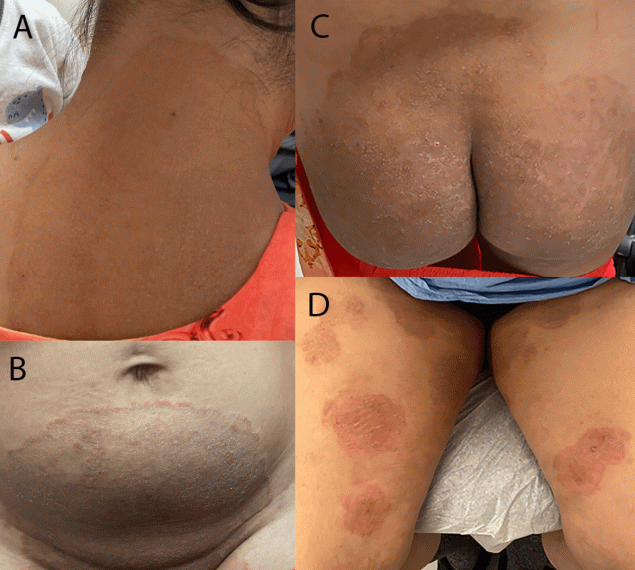
Image Gallery: Widespread erosive tinea corporis mimicking autoimmune bullous dermatoses in a patient with lung cancer - Shen - 2020 - British Journal of Dermatology - Wiley Online Library





:max_bytes(150000):strip_icc()/VWH-DermNetNZ-AthletesFoot-02-bb8f567595ac4435a7d7a190c12d05a9.jpg)
:max_bytes(150000):strip_icc()/ringworm-overview-2632044_FINAL-e1669cad90b347b981a4c1ae42865fcc.png)